Information
Advanced Procedures
Adrenalectomy.
Small tumors of the adrenal glands can be completely removed by laparoscopy. It is a procedure that consists of removing the gland very effectively and with minimal pain. The patient recovers quickly and is discharged one day after surgery. Unlike the pain caused by open surgery, this method almost completely eliminates it and greatly improves the aesthetic sequelae produced by a lumbotomy or laparotomy (open surgeries). It only requires 4 small incisions.
See video: Right Laparoscopic Adrenalectomy for Adrenal and Kidney Cyst.
Laparoscopic Bypass.
This is the name given to the union of the small new stomach that results from obesity surgery with the small intestine. This is done with a manual technique with an extracorporeal knot (outside the body) and is very safe given the characteristics and support of this type of knot. At the end of the procedure, the patient eats very little food and the little that he eats is absorbed very little, so he loses weight quickly and safely, helping to eliminate diseases such as diabetes and high blood pressure in many cases. Strict monitoring is required after surgery by a surgeon specializing in bariatrics.
Watch video: joining the new stomach with the intestine (bypass)
Appendectomy for complicated appendix.
Some cases of appendicitis can be very difficult even in an open procedure. Laparoscopy minimizes the possibility of complications derived from an open procedure in advanced and complicated cases of acute appendicitis. This is based on the almost perfect visualization of the anatomical structures involved in the inflammatory process, minimizing the possibility of a bad evolution due to early detection and repair of the damage. (Difficult to achieve with open surgery due to the limited incisions). It practically eliminates the possibility of wound infection because the procedure is controlled and because the piece contaminated by batteries is removed through a tube that prevents contact of these waste tissues with the surgical wound, thus avoiding a viacrusis for the patient due to an infected or dehiscent wound (open due to poor tissue quality). Finally, it reduces to a minimum the possibility of single or multiple abscesses or pus collections since it allows a more complete cleaning and irrigation of the abdominal cavity than traditional surgery. It can be performed even in the most difficult cases of appendicitis.
Watch video: Appendectomy with abscess and fusion with uterine tube
Pancreatic pseudocyst derivation.
Some patients who suffer or suffered from inflammation in the pancreas due to stones (lithiasis) or increased blood fat (pancretitis) can develop what is known as a pancreatic pseudocyst (false pancreatic cyst) since it does not contain a true wall. These false cysts can grow so large that they cause abdominal pain and, in later stages, nausea, food intolerance and vomiting, with secondary malnutrition and death. This problem can be resolved by laparoscopy. A connection is made between the false cyst and the intestine, causing drainage of its contents into the intestine and, over time, its disappearance with an excellent quality of life.
See video: Cystojejunostomy
Drainage of ruptured pancreatic pseudocyst.
In some cases, false pancreatic cysts rupture and cause abdominal pain and abdominal chemical peritonitis. It is possible to safely inspect, identify, drain and unroof the false cyst by laparoscopy. This prevents the damage from continuing and eradicates the intestinal inflammatory focus. In many cases, the patient no longer requires a second surgery for control. Minimally invasive access contributes to a quick recovery and does not increase the abdominal inflammatory damage, leading to the patient’s prompt return to work.
See video: Drainage and unroofing of secondary collection due to ruptured pancreatic pseudocyst
Splenectomy.
In some hematological or blood diseases where red blood cells (anemia) or platelets are drastically reduced, it is necessary to remove the spleen, a solid organ located on the left side below the last ribs, which acts as a filter that reduces the count of these cell lines. Removing this “filter” or spleen by laparoscopy (laparoscopic splenectomy) significantly increases the platelet and blood cell count, contributing to the improvement of the patient’s clinical condition and reducing or eliminating the number of transfusions and bleeding that these people have. The laparoscopic method is a very safe, aesthetic, painless method and helps reduce the complications so common in open surgery (open splenectomy).
Watch video: Splenectomy or removal of the spleen
Removal of the gastric band.
When the adjustable gastric band, used in obese patients for weight loss, no longer helps to lose weight and begins to cause problems in the upper digestive tract (bleeding, closure of the stomach, reflux, erosions, Barett’s esophagus or precancer, gastric perforation or penetration) it is necessary to remove it. Removal is preferably performed by laparoscopy. It can be as easy or as difficult as it is attached or glued inside the abdomen to the stomach and adjacent viscera. The ideal method for its removal is laparoscopy. This method provides the best functional and aesthetic result for the patient.
Watch video: Gastric band removal
Laparoscopic gastric sleeve (sleeve gastrectomy)
Laparoscopic sleeve gastrectomy is one of the most modern and functional methods for weight reduction in morbid obesity. Initially it was proposed as a temporary method or first procedure to help with weight loss but currently it has been seen that the results of excess weight loss are as high as 70% of the EPC. It is a restrictive method although it also has a certain hormonal component to reduce a substance in the blood that is produced in the gastric fundus that produces appetite in humans (Ghrelin). It is ideally performed by laparoscopy for the convenience of reaching the deepest part of the hiatus. It is a very safe method in expert hands. It requires four small holes for its execution. The patient is discharged from the hospital two days later with a liquid diet. Watch video: Sleeve gastrectomy for morbid obesity.
Gastroyeyunoanastomosis.
In cases where the patient accidentally or voluntarily ingests toxic acidic or alkaline substances and/or in patients with benign tumors that close the terminal part of the stomach and prevent the passage of food into the intestine, a gastrointestinal bypass is required to allow the gastric juices and food trapped in the stomach to pass through. This procedure is called gastrojejunal anastomosis. It can be performed successfully by laparoscopy. The patient’s recovery is impressive and he or she can eat again within a few days of surgery. In these patients, nutrition is very important to achieve adequate intestinal healing, otherwise the risk of fistulas or leaks and complications is very high. The procedure can be performed with a stapling system (mechanical gastrojejunal) or with extracorporeal suture (manual gastrojejunal). Both are very effective methods. The patient returns to his or her normal life in a few weeks. Watch video: Mechanical gastrojejunostomy
Watch video: Manual gastrojejunostomy
Right hemicolectomy for tumor (laparoscopic right colon resection).
Certain conditions such as complicated appendicitis that cause damage or rupture of the large intestine (part of the colon called the “cecum”), tumors in this same location and/or colon diverticula can be resected (removed) by means of laparoscopy. This method causes excellent recovery despite being major surgery. Laparoscopy avoids complications that are more frequent in open surgery and achieves great abdominal aesthetics with prompt reintegration of the patient into social life.
See video: Right hemicolectomy for tumor of the cecum (right colon)
Inguinal Hernioplasty.
Abdominal wall hernias are resolved safely and effectively laparoscopically. It is a controversial method due to the technical difficulty it presents, becoming a challenge even in expert hands, mainly in recurrent hernias (hernias already operated on that failed by open technique) since they present fibrosis or adhesions due to the lack of “virginity” of the abdomen. Laparoscopic hernioplasty is a very safe and cosmetic method. It is ideal for medium and small hernias and mainly bilateral hernias of the inguinal canal, where both hernias (left and right canal) can be repaired with a single approach. It is possible to repair any type of abdominal wall hernia by laparoscopy with only three small 0.5mm incisions.
Watch video: Laparoscopic Inguinal Hernioplasty
Myotomy for esophageal achalasia.
There are certain esophageal conditions that prevent the normal passage of food to the stomach, which causes weight loss and, in severe cases, malnutrition of the patient with secondary death. One of these problems is esophageal achalasia. The current treatment for this condition when pharmacological and endoscopic measures have been exhausted is cutting the muscle fibers at the level of the cardia and lower esophageal sphincter (esophageal cardiomyotomy). With this procedure, the patient returns to his normal life a few days after surgery, gaining weight and nutrition, recovering all the organic functions lost in this type of patient.
Watch video: Laparoscopic cardiomyotomy for esophageal achalasia with scissors
Watch video: Laparoscopic cardiomyotomy for esophageal achalasia with harmonic scalpel
Esophageal surgery
Esophagectomy
Esophageal surgery, known as esophagectomy, is a surgical procedure primarily used to treat esophageal cancer and other serious esophageal conditions, such as Barrett’s esophagus and advanced-stage achalasia.
What does esophagectomy involve?
- Removal of the esophagus: Part or all of the esophagus can be removed. In some cases, part of the stomach and nearby lymph nodes are also removed.
- Reconstruction: The esophagus is reconstructed using a part of the stomach or, in some cases, a section of the intestine.
Esophagectomy techniques
- Open esophagectomy: Performed through large incisions in the neck, chest, or abdomen.
- Minimally invasive esophagectomy: Uses laparoscopic or robot-assisted techniques, which can result in less pain and faster recovery.
Risks and complications
- Respiratory complications: Such as pneumonia.
- Infection and bleeding.
- Digestive problems: Such as reflux, nausea, and difficulty swallowing.
Preparation and recovery
- Before surgery: It may be necessary to stop smoking and adjust medications. Preoperative treatments such as chemotherapy or radiotherapy may also be recommended.
- After surgery: Recovery may include a prolonged hospital stay and medical follow-up to manage any complications.
Laparoscopic Cardiomyotomy
Laparoscopic cardiomyotomy is a surgical procedure primarily used to treat achalasia, a condition in which the lower esophageal sphincter (LES) does not relax properly, making it difficult for food to pass from the esophagus to the stomach.
What does the procedure involve?
- Laparoscopic access: Small incisions are made in the abdomen through which a camera and specialized surgical tools are inserted.
- Myotomy: The muscle of the LES is cut to reduce pressure and allow food to pass more easily into the stomach.
- Fundoplication: In some cases, a fundoplication (wrapping the stomach around the esophagus) is performed to prevent gastroesophageal reflux.
Benefits
- Less invasiveness: Compared to open surgery, laparoscopy offers less postoperative pain and faster recovery.
- High efficacy: Significantly improves symptoms of achalasia, such as dysphagia (difficulty swallowing).
Risks and complications
- Infection and bleeding.
- Esophageal perforation.
- Gastroesophageal reflux.
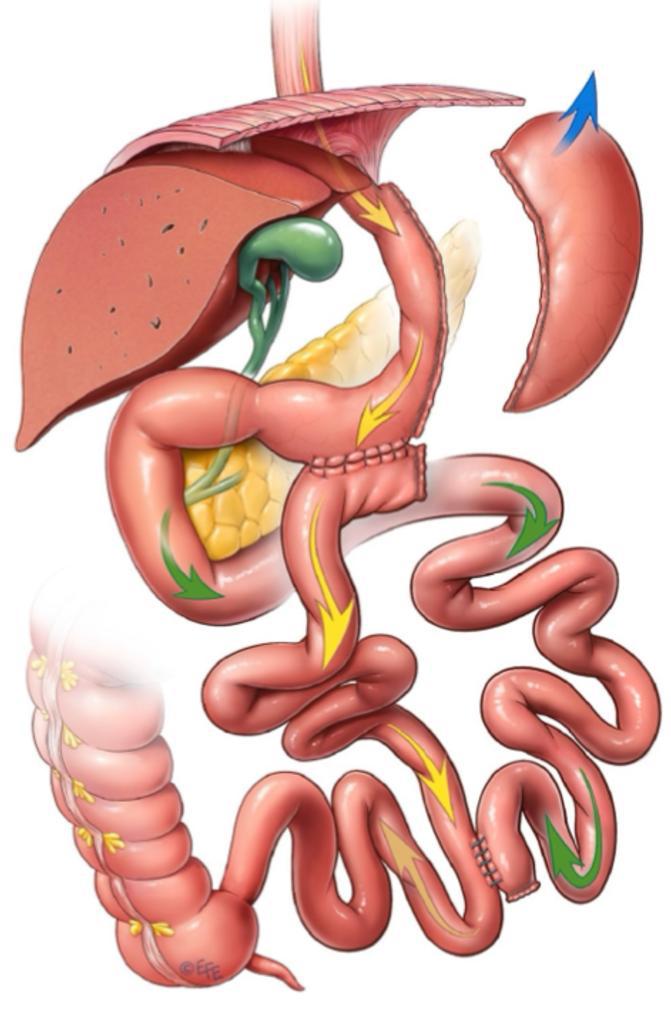
Bipartition of intestinal transit
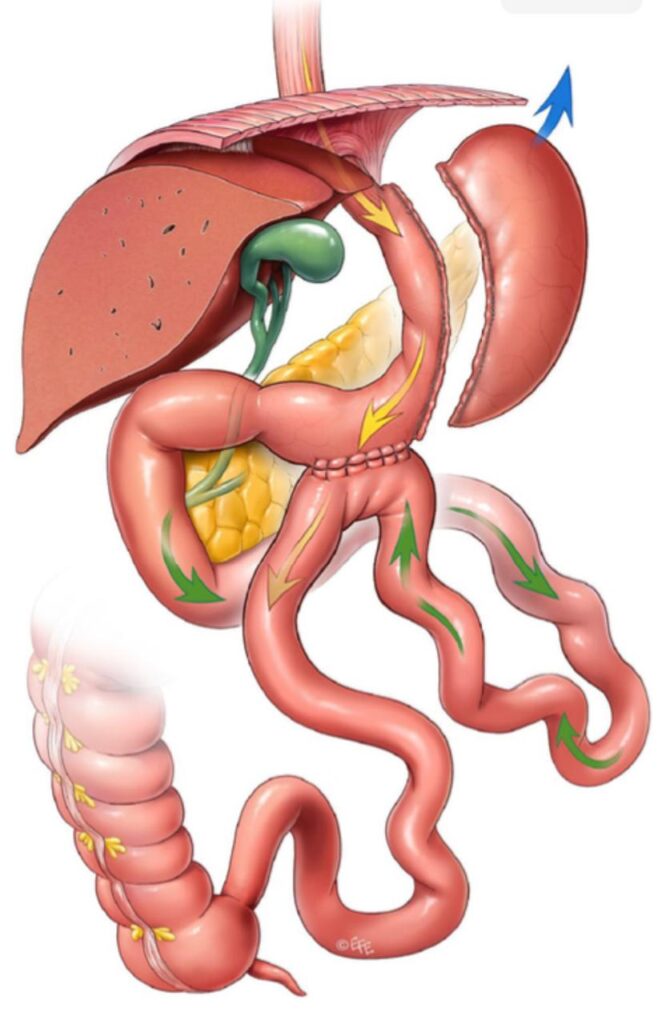
BTI is a metabolic-bariatric surgery technique that involves creating two pathways for food to bypass part of the small intestine. Bipartition of intestinal transit is a surgical technique that has revolutionized the approach to obesity and type 2 diabetes. It consists of a reconfiguration of the small intestine, dividing it into two segments. This anatomical modification induces physiological changes that promote weight loss and blood sugar control.
Physiological bases:
- Increased secretion of incretins: Incretins are intestinal hormones that stimulate the release of insulin and reduce the production of glucagon, which improves glycemic control (current medications for diabetes and weight loss arose as a result of this type of ileal surgery (due to its anatomical confirmation towards the terminal ileum).
Increased exposure of the intestinal epithelium to bile acids: This modification alters the absorption of fats and favors the feeling of satiety.
Modification of the intestinal microbiota: The new intestinal configuration influences the composition of intestinal bacteria, which can contribute to weight loss and improve metabolism.
Advantages over other procedures:
- Greater simplicity: It is a less complex technique compared to other bariatric surgeries, resulting in shorter surgical time and lower risk of complications.
- Better metabolic outcomes: Studies have shown that intestinal transit bipartition is highly effective in the remission of type 2 diabetes and in sustained weight loss.
- Lower risk of malabsorption: Unlike other techniques that can cause severe nutritional deficiencies, intestinal transit bipartition usually preserves the absorption of essential nutrients.
Bipartition of intestinal transit is a promising surgical option for the treatment of obesity and type 2 diabetes. Its mechanism of action is based on physiological modifications that promote weight loss and glycemic control. The simplicity of the technique, together with its excellent results, position it as an attractive alternative to other bariatric procedures. Schedule your appointment to learn more details.
Travel plans
Learn how to schedule and plan your surgery
We offer excellent accommodation and travel plans so that you do not have to worry about anything when it comes to your surgeries or treatments.